
Arthur is not self-aware that he does not know how to stage a pressure ulcer which is a limiting factor for his skills to communicate as a nurse.
Heroes Acknowledged
"That's ridiculous." Tim owns and runs a mobile radiology company and I had just sent him a text to tell him that a major home lab had suspended home phlebotomy. I wanted to check in to see if NY Home X-ray had done the same. The lab eventually reversed their initial panic protocol and resumed in-home phlebotomy, but NY Home X-ray never panicked. Tim's meta-message was right. If you are in health care and act ridiculously when your services are needed most, then you shouldn't be in health care.

Yesterday, the heroism of the work this mobile radiology crew is doing hit me more so than our first text exchange weeks ago at the start of our era of sirens. Tim himself was out in the field on a Sunday suited up to protect himself and my vulnerable home bound. He doesn't always call, but yesterday he did call to read the radiologist's report because it was abnormal, "viral pneumonia," "ground glass," "COPD." We talked about his crew of radiology technicians. No, none of them had become sick with novel coronavirus. I asked how they accomplished that despite a month of frequent exposure opportunities. Tim described a well thought out and detailed equipment use protocol. He told me about all the gear. He said he had plenty of protective equipment. Preparation is the foundation of a goal to provide continued service. "We have to get in and out." I have been in the home with them in the past. Tim's radiology techs are usually calming, social and chatty. They have always helped the sick patients feel comfortable so they can lay on a hard cold x-ray plate, but in our era of sirens, they can't linger anymore.
Yesterday Tim described how he knows when it's coronovirus. Radiology techs can't read x-rays, but they look at them. They have to look at the screen to make sure they got the picture which captures the truth in the same way you do with your camera. After years they come to know abnormal and they come to understand something about how the official reading of the radiologist fits the image that they saw on screen together with the real person whose picture they took. Radiology techs see both the image and the experience of the patient. The radiologist only sees the black and white image. Its coronavirus if the normal black of the lungs are more white where they should show more black and also if there is fear in the eyes of the patient.
"Stay home if you are sick," our leaders and experts say. There are very few of us to help those who are staying home with fear in their eyes. Yesterday, Marie who found me on the internet, said she had been calling her doctors plural and received no call backs from messages left on Wednesday, Thursday, Friday and Saturday. So much for the satellite hospitals of prestigious medical centers having available telehealth services. She was relieved that she had enough medications for her chronic conditions. She thought she was calling me for the kind of pneumonia that she barely survived seven months ago. She has coronavirus. I knew that was her diagnosis when I left her apartment. Just hours later Tim confirmed my impression when he read the abnormal report and also witnessed the fear in her eyes. She will never make the statistics unless she dies from it because I can't test her, so just add one to the stats of positive.
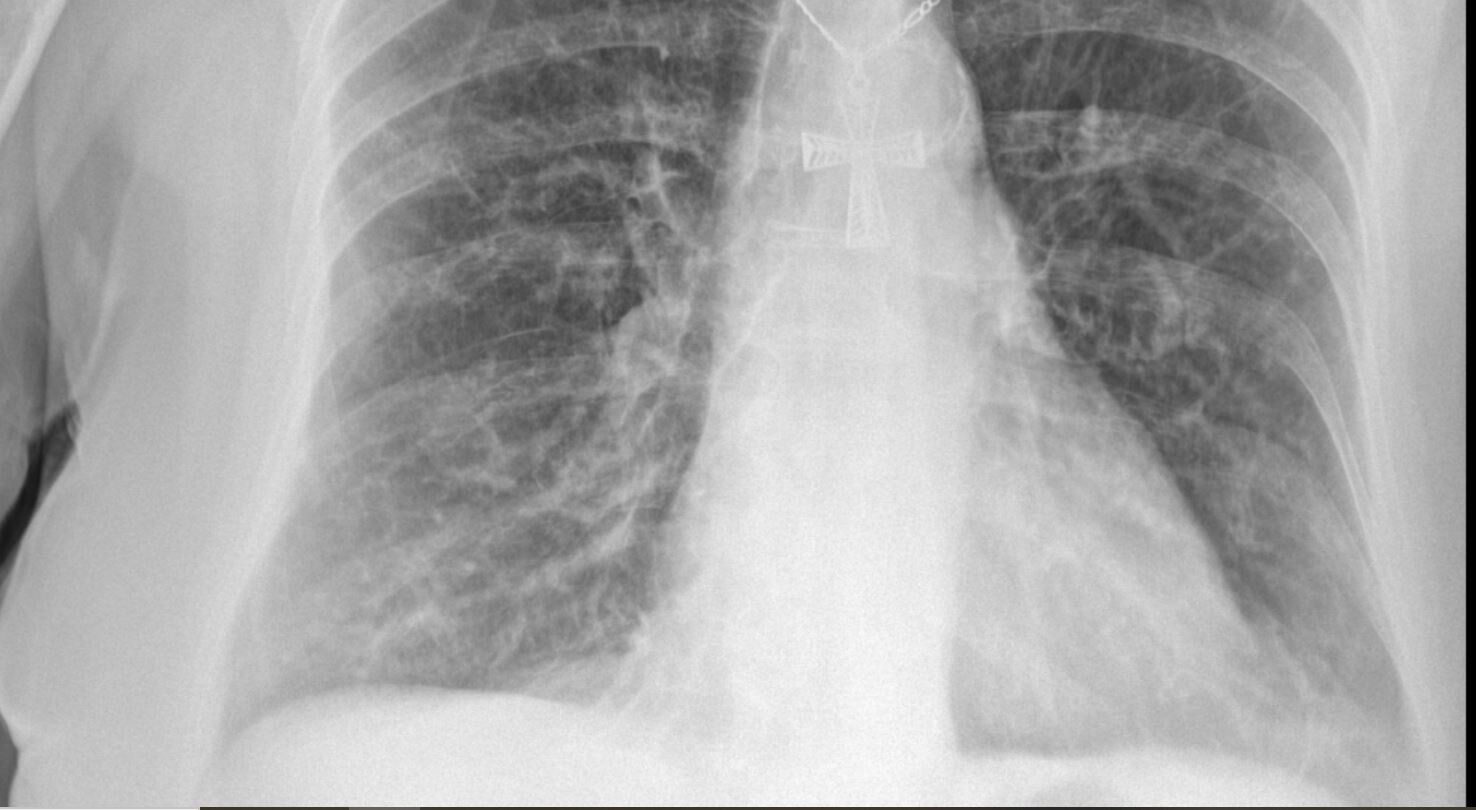
It is notable that the heroes of NY Home X-ray were prepared and protect themselves so that they can help me make a diagnosis one step beyond a pretest probability. Its a pandemic, by definition the pretest probability is off the charts, but the symptoms and abnormal findings can be other common diagnoses. Tim and NY Home X-ray help me determine that it is or is not something else. "Stay home if you are sick" is a more than a little "ridiculous" if your needs are a diagnosis and available doctor to mitigate the aloneness and fear. I appreciate the heroes of NY Home X-ray for generating the image that helps me help those who are told not to go to a hospital. They deserve to know too.
The 30th Precinct does Elder Abuse Well

What officers from New York City 30th precinct did, they did with empathy, sensitivity, and considered deliberate decision-making. They arrested a home health aide at the end of her shift for elder abuse. Well, the “elder abuse” umbrella term in my vernacular isn’t a crime, but specifically larceny wrapped up with fraudulent use of an elder’s federal entitlement food stamp benefit is a very serious crime.
I called 911 for an unaccounted for food stamp card charge of $13.19 which occurred four minutes after the $15.55 legitimate purchase matching the items on a 94 year old woman’s handwritten grocery list. It wasn't my idea to call 911 for what is not fire, chest pain, or blood on the floor, but the 30th precinct officer who interacts with neighborhood elder abuse advised me that this required officers on the scene; the business card of her predecessor was already in the elder's home. And so I called 911 after Fatima, the home health aide who had the food stamp debit card and the PIN, but no receipt, denied making any other purchases. It’s easy to verify date, time, and location of a food stamps debit card purchase, even the victimized elder knew how to call the number to listen to the automated account history. By the time I called 911, I reached the opinion that Fatima used the food stamps debit card once to buy the elder's groceries and a second time to buy herself exactly $13.19 of groceries to take home. She left me no room for doubt.
I called the police after I left the apartment and also after I called Tender Care, Fatima's employer. Neither Fatima nor Tender Care expected that I would go back to the home where the story was being revised. By the time the responding officers arrived and I returned, a bag of groceries and a receipt had appeared, maybe both were discovered after a call from her employer prompted her to find them. Now Fatima changed her previous statement from "No. I didn't buy anything else," to "She told me buy them. She called me while I was in the store." The two young responding officers from the 30th precinct heard everyone express their viewpoints with respect. They encouraged the accused to give her version of the grocery charge. They allowed the victim to eat dinner in her worn house dress while she repeated “I didn’t tell her to buy that,” and "I don't eat that." They gave me, the irate advocating home visit doctor, a voice to the “larger implications for all other old people.” I reported that after I called Fatima's employer, she tried to make the victim whole by tossing $20 on the kitchen table and asked for change.
These first responders were realistic. They said the District Attorney was unlikely to want to prosecute. They understood that the situation was perp's word verses victim's word. Even more importantly, they understood that old people have an additional credibility barrier because even when they can give details about the televised royal wedding in response to a memory question, someone is going to claim they "forget," "forgot," "don't remember" or "are losing it." When the young responding officers failed in their empathetic negotiations, they had to called even more senior officers to approve putting a home health aide in hand-cuffs. A sergeant and seasoned officer arrived and continued to search for a resolution which didn't involve arrest.
A small piece of what I call elder abuse includes the crimes of taking money out of wallet or bank account, or in this case the government entitlement assets of an old person. Think about that. This strong word abuse is used when a few dollars or social security check is stolen inside the home by a grandchild or a home care worker. To most people a pickpocket on the subway is a bigger crime and a more obvious call to 911. But what is the difference? The only difference is the pickpocket is a stranger in an admittedly dangerous world. What does domestic theft between intimates have in common with pickpockets in the outside world? It’s not an isolated incident. The home health aide who successfully makes off with $50 in cash or $13.19 in groceries has thieved an elder before and will do so again. From the victim’s point of view, the pickpocket is random crime by an anonymous bad person, but a theft from a home health aide or family member actually does leave bigger bruises and more permanent scars. It has longer lasting effects of victimization on elders who know they need help, were failed by trust and are now proven to be unsafe in their own home. That's why abuse is an appropriate word.
Fatima was arrested in the kindest way possible. The elder felt the advocacy around her. Based on the exemplary actions of these five officers from the 30th precinct, I felt that perhaps my microcosm world of the homebound in New York City had one less serial elder abuser. The 30th is my home precinct, so on a closer-to-home level, I hope they keep up the good work for the next 30 years which will be when I will need them to advocate for me.
The Cost of a Bag of Groceries

I see elder abuse all the time, but today was the first time I saw a home health aide taken out of a home in handcuffs. I see elder abuse frequently, often, and in all its variations, but rarely do I have the circumstances to do anything about it. ARC left me a message about sending "the lady, her name is Fatima," a new home health aide from Tender Care, to the supermarket “to buy four things.” When Fatima came back with the groceries, ARC noticed the remaining balance on her food stamps debit card was reduced by more than the cost of those items.
I met ARC in about 2006 as the caregiver for her husband who was my patient. She negotiated all the tasks of her husband’s care well. She became my patient in 2013 and during our relationship she has remarked on not believing her own age. She has often shared the values imparted by her rural subsistence farmer-preacher grandfather about telling the truth and work ethic. ARC and I have had many conversations about "people stealing from my wallet," and "I am just a trusting person," "I don’t have anything, why do they take advantage of an old lady?" Around the time she turned 90, I posted a big hand-written sign on the mirror at her kitchen table with the single word VULNERABLE. I wanted her to be reminded of her predicament. One day she asked a physical therapist to add the meaning of vulnerable to the page, so I know she was thinking about it. On this same mirror she has a laminated sign with the phone numbers to report elder abuse to New York City Department of Aging and the business card of the officer at the 30th precinct who deals with all the vulnerable old people in her neighborhood. Her kitchen table mirror displays these three reminders intended to avoid another encounter with elder abuse. I have had many conversations with her about scams that might come in the mail asking for money, and people who call on the phone to invite themselves in to her home for valid or not so valid reasons. She had not been so savvy about acquiring the names, titles and agencies as long as these people were nice. My instructions to her start with the context of how much the world is a different place than when she came into it nearly 95 years ago. I always say “It’s not you, but you are unable to keep up with the way people conduct themselves these days.” I then tell her to call me or her niece if a stranger makes an offer or takes advantage.
Today, she pulled self-advocacy out of that innate vulnerability. Yes, she did the math and the cost of groceries purchased from her shopping list subtracted from the previous balance left today’s remaining balance on her food stamp debit card less than it should have been, so she called me. I suppose it would be fairly easy to get away with stealing a few bucks from the wallet of a senior while they aren't looking and blame it on their memory deficits. In fact it happens all the time, but to use a digital food stamps debit card to make a purchase that is ridiculously traceable. Fatima surely saw vulnerable, but not the certain cost to herself because every charge on the food stamps debit card records location, date and time. With both of them watching, I used the printed receipts for the month and sequentially subtracted next purchase from preceding balance to find the discrepancy. ARC was right ten or so dollars was not accounted for by receipts on the kitchen table. She knew exactly how to call the automated system that recites every deposit, purchase and refund on her food stamps debit card. I listened to it twice for date and amount. Indeed, in addition to the purchase for the groceries Fatima put in the refrigerator, today there was another separate purchase for $13.19 a few minutes later. Fatima said she had no other receipts and made no other purchases. Nope, she knew nothing about it even after I asked again, rephrased and repeated. She was the only person holding the food stamps debit card and the PIN when those purchases were made. When I called her employer in front of her, she pulled out a twenty dollar bill and threw it toward me on the table and said to take the money out of it, "do you have change?" and she said the same to ARC, “take it and just give me the change."
Fatima ultimately walked out in handcuffs, but that only happened after I left ARC’s apartment and her employer called and told her to make copies of the receipts. Apparently he didn’t trust my math. Jonathan who claims to be the boss at Tender Care accurately predicted that "maybe the groceries would be found in the apartment." While my elder abuse alarm was at full blast, Fatima’s employer was extremely certain that there were oh so many explanations and that the next step was to find a missing bag of groceries by searching in the apartment. At the time I thought his hypothesis, that I would find another bag containing $13.19 worth of groceries, was ridiculous because Fatima said she had no other receipt and ARC’s hand-written shopping list was clearly just four items. In retrospect, it seems that this home health agency had been through this before. In other words, when an unexplained charge on a food stamps debit card is discovered before end of shift of the employee doing the shopping, the resolution is: How considerate of her to pick up a few extra items and safely store them behind the sofa. All is well. It’s so lovely of her home visit geriatrician to help us find them.
The police were there when I returned to the apartment because I called them, so was a receipt for $13.19 and a bag containing banana cake mix, cake icing with sprinkles, a 5 lb. bag of flour, two peaches and two plums. Not only does ARC not bake because she can't stand in the kitchen and her hands are badly affected by arthritis, but neither does any other 95 year old. So, Jonathan was right the missing groceries were in the home, but they weren't items on ARC shopping list and they weren’t food she eats. Most importantly they materialized after a grocery bill didn't add up. The police gave Fatima every opportunity to do three things: just admit she bought groceries for herself with ARC's federal entitlement dollars; apologize; and return the items, but she wouldn't. Her story got more convoluted and contradictory. She said ARC called her while she was at the store and told her to buy items that she doesn’t eat. The home health aide insisted that the vulnerable old lady directed her because all home health aides know their job exists exactly because of vulnerability. Why two purchases? Why did the receipt and groceries appear after I called her employer? Why was there no record of the call on her phone? Oh, because ARC doesn’t actually have Fatima’s phone number and didn’t call her to make the second purchase that was denied when I first arrived. The story didn’t stick with five police officers sensitively seeking an honest admission, apology and grocery refund. Fatima left the home of a self-advocating old lady with a cost to herself of much more than $13.19. She left in handcuffs.
Nobody Asked

I asked an attorney friend of mine who teaches other lawyers about guardianship matters how I can write a letter to the judge about loose ends in a guardianship. Her reply was, "I wouldn't because it's done and nobody asked."
Well, the loose ends are that nobody asked. Law and justice sometimes interface with health care. Guardianship involves mental health, keeping up with medications, preventive health, and making crucial decisions in a hospital. Questions about health and health care cannot be left as loose ends at the time of judgment. People who need guardians by definition are marginalized and more often than not have serious health issues around which they themselves cannot self-advocate. The average observer holding the scales of justice is blindfolded to the medical issues.
I left the courtroom at 60 Center Street, specifically room 355, officially ambiguious. There was the former doctor sitting behind me who had been dismissed for failing to provide nursing care to a pressure ulcer for one year, failing to communicate with a health care agent, failing to tell everyone that the skin cancer she scraped off was still in the skin and would come back, and failing to give the flu vaccine to an old bed bound person. It was official in the court record that she could visit the patient as a friend because the old bed bound person, a ward of the court, likes her so much. I also heard say the judge that the current doctor should be replaced with an "independent" physician but no such “independent” physician was identified in courtroom 355 on Friday at 4 pm. Neither was the appointed guardian in the courtroom. Only five lawyers could raise their hands and asked for "specific language in the settlement" and "clarification about a co-guardian," advocating for their clients. Left loose and off the record was a provision for health care on Friday at 4 pm. I have been providing her health care 24 hours no matter business, lunch or after hours, but I wasn't given the last name or phone number of the guardian. I know him as "cousin Sam." The most I could do was to give my card to "cousin Sam's" attorney, but she didn't give me hers. My patient's appointed attorney took my card, but said she didn't need to know me the reason being that she is the old bed bound person's lawyer and apparently not her advocate.
I woke up Friday night with a nightmare that my bed bound patient who has no fat padding rolled out of bed on to the linoleum with an INR of 3.4 and the home health aide called for blood on the floor, but it was only a dream that I could not notify “cousin Sam” that I had sent her to the nearest ER unconscious or that I had sent a fax of her medical conditions and lab report to the hospital. What isn't a dream is that tomorrow while the guardian and his attorney might have time to take up the search for an "independent" home visit physician during business hours, the nurse coming to do wound care will have run out of the state of the art wound care supplies for the bedsore and the ambiguously current geriatric care manager has no access to funds to order more of them and she doesn't know the guardian either.. And if the guardian and his attorney haven't found an "independent" home visit physician a week from now, the seven-day-four-slot pill box with mission critical medications will be empty and the home health aide won't be able to cue the bed bound patient that it’s time for the before breakfast pill, the after breakfast pill and the after dinner pill too.

The official court record does omit addressing if everyone who has an ethical obligation to stay involved has adequate access to everything that they need to meet the 24 hour needs of the bed bound person. The official court record says that the former physician can come over to play chess because the patient requested that, but "nobody asked" if the ambiguously current physician and new guardian know how to contact each other. Justice sees the guardianship as “done” while medicine sees the ward of the court as being invisible to the blindfolded.
Rose died with all of her marbles

Rose died today with all her marbles. Anyone who knew her can hear her say it with that hard-to-place European accent. "I've got all my marbles," as she pointed to her temple with a wink. Metaphoric marbles are a point of competitive pride with anyone over ninety, but hardly anyone who is 94 and six months gets so lucky as to die with all of them. Rose was in a coma or near coma for only the last 16 hours of her life, but that and morphine don't count for lost marbles because earlier this week she told me the date of her granddaughter's husband's annual colonoscopy as if she simply had to keep track of it for him. The day before today she told me her sweater was cashmere and gave me exacting instructions on how she washed and ironed it in order to keep it looking like new for the last 10 years.
I met Rose in 2009 when her primary care physician left the area and her pulmonologist referred her to me. At the first visit I was tested. She asked about why she needed to take medications if she didn't have the illness to go with them. She couldn't make sense of why one doctor prescribed a diuretic and another switched it to a different one without explanation.. She wanted to know how smart I was and to find out if I would attribute her concerns to "old age." She treated the first office visit like a first date and sized me up to see if we had longevity potential.
Rose wasn't going to be one of those people who leave the last choices of her life up to others. This was between her and me minute by minute. Besides reminding everyone that "when it’s your time, it’s your time," she carefully left her sons out of explicit acknowledgment of prognosis. She didn't ask me for prognosis either, but instead read my face for silent information, the same way I read hers for how much moral and mental energy she had left to get through the irreversible deterioration of her physical being. I can't recall ever seeing a body die day by day for weeks without losing any marbles despite worsening in the number of things that doctors measure. Rose and I had a secret language. I can't trace the origins of it, but it got us through at least four health crises with return to quality of life. What is a doctor if not a partner during life and near misses?
Rose died hours after a quick bed bath and change of night gown because all three of us who were there knew the morning routine. She died under her daughter-in-law's purple-turquoise hand knit cashmere throw. Before her sons arrived her companions giggled the secret story of Rose instructing them to practice Kegel exercises as her public service reminder to aging women everywhere. Practice makes perfect to prevent incontinence. The granola-baking granddaughter was there to repay mothering with a song of love. Another daughter-in-law physician accepted responsibility for titrating morphine to life without symptoms. I was with Rose almost every day in the last two weeks as her body deteriorated and despite the symptoms, eye to eye we both pointed our finger to our temple and said the word "marbles."
Ageism is negative and depressing
Today I went to a meeting for the Radical Age Movement where people in their 60s and 70s, all of whom were working, articulated their experiences with ageism and why the old are the last group left to face discrimination. All other marginalized populations have had their shifting views movements. I heard how a professor can not say to himself or others that he attributes his skills at being effective to his age. I heard that being offered a seat on the bus evokes widely different emotions and actions. I think this organization will use the experiences of people currently in their 80s and 90s to change the perceptions of age, disability and community of care fast forwarded 20 years.
Today I got email from someone who was trying to connect me to the senior services for an extra large apartment complex in New York City where people have aged in place. The feedback from the director of the senior program was that the images of old people on my business card are "depressing" and that I should say that I make "house calls" instead of provide accessible care for the "homebound" because that's "negative." I think that the reason that the homebound elderly are invisible is not because they can not leave their homes but because many people choose not to acknowledge them.
Dr. Odd and Ms. Vulnerable take on UnitedHealthcare

On Wednesday I was called by a representative of Ruth's insurance company, UnitedHealthcare, to request lab results. Yes, her health insurance company wanted in. They wanted to look at the control of her diabetes with no context of our private discussions about her diabetes. Apparently, UnitedHealthcare is on a parallel track to reach some lab goals on paper for a woman who is 90 years old. Ruth and I have our own goals for her health. A nameless, woman wanted to send a written request for specific labs, she emphatically claimed that Ruth signed a paper authorizing permission for me to send the results. I told the anonymous representative of the mega-for-profit organization that it was unlikely that she was giving informed consent for them to get into the doctor-patient relationship, furthermore that if she had signed something, I would see that she revoked consent to send them anything. The person on the other end of the phone said, "You sound odd," and hung up.
I called Ruth and asked if she signed papers for me to send lab results to UnitedHealthcare and she said, "No."
Then Ruth and I reviewed the instructions which I had given her many times before after she let seemingly well-meaning people with no names into her home. Don't let anyone in your door without calling me or your step-son, and don't sign anything no matter how nice the person seems.
I said, "You are vulnerable old lady." "You think so?" she squealed. Then answered her own question giggling, "I guess I am!"
Within minutes of hanging up on Dr. "Odd", the anonymous representative of UnitedHealthcare called Ruth to invite herself for an apartment visit on Friday. Ruth initially said yes to the still nameless woman from UnitedHealthcare, but then remembered my instructions from five minutes earlier and called me back to get her phone number so she could cancel the reconnaissance mission. Ruth and I think that her health insurance company is crashing our doctor-patient relationship. I wonder what they can do to improve Ruth's health with just a number on paper and without knowing all the things I know about her.
When she gets this way, I feel I have to do something

He is a baby-boomer son who for years got his mother the best possible medical care. It’s not that he made her decisions for her, but he found the best evaluation and she weighed in with the yes or no choices. Together, they got through some complex surgery. They dealt with months of adjusting medications to treat side effects of other essential medications. When he found me, it was to address an acute respiratory infection, and then he told me about the urinary tract infections which "occurred like clockwork every month." Because she was homebound, a dedicated specialist working outside his area of medical expertise, in effect filling a void in access to primary care, was authorizing a urinalysis monthly. And every month she also had sudden urges to urinate, mild leakage of urine, false alarms of getting to the toilet with an empty bladder, as well as cognitive lapses, minor paranoia and transient disturbance of personality. Her son was now rightly concerned about combining the antibiotic for the respiratory infection with the antibiotic for her "like clockwork" urinary tract infection. Me too. When I received the urine culture and urinalysis results collected in the past two months, and knew the context of how the urine was collected, it was clear that any bacteria which got to the lab were from her skin or the plastic commode bowel.
Her son had a hard time accepting that the antibiotics he gave her were not treating an infection because her sudden urges to urinate, mild loss of urine, false alarms of getting to the toilet with an empty bladder, and fluctuation of mind were perceived as getting better because of the antibiotic. He said, "When she gets this way, I feel I have to do something."
This is a common mistake doctors make too. It’s not what we can do; it’s what can be achieved. We can cure an infection with antibiotics if it’s the right antibiotic. We can avoid very serious side effects, medication interaction, and future bacterial resistance if we don't give antibiotics when there is no infection.
The focus for caregivers should be achieve something instead of do something.